There is a famous person who really should be a lot more famous, even after having earned the Nobel Prize in Physiology or Medicine in 2015. Her name is Tu YouYou. She discovered artemisinin, which is now the first line malaria medication for infected cases. What's even more interesting and perhaps more deserving of fame (in light of the result of course) was that she did so by mining traditional medicine systems, in this case Traditional Chinese Medicine, to find this therapeutic. This is one of those medications that are probably most easily and appropriately termed a 'cure', although the medical profession looks down at that term for anything because of the expectations it instills in the patient and their loved ones (and there's always an exception, complication, or side effect in some small number of patients relative to the total number of treated).
Anyway I was at the KEnya Medical Research Institute hq the other day, in their Traditional Medicine Research department. There was a binder there from 2002 with the agenda and speeches from an Africa-China traditional medicine research convocation in Beijing. There was a speech of hers inside, and I was given permission to transcribe it. Here it is:
"
China-Africa Forum on Traditional Medicine convened from 20-22 October in Beijing
Qinghaosu [ed. note: Artemisinin] - the Crystal of Traditional Anti-malaria Chinese Medicine
Tu Youyou
Director, Research Center for Qinghao and Qinghaosu, China Academy of Traditional Chinese Medicine, Beijing, 100700, China
I am a researcher from the China Academy of traditional Chinese medicine. Traditional Chinese medicine (TCM) with its unique theory is shaped from the long history of medical practice and experiences accumulation of the Chinese nation. TCM protects the development and multiplication of the nation. THe flourishing of TCM today is based on the continuous invention nad innovation in its history. In 11th century BC, anatomic terms of human body and descriptions of a number of diseases were recorded by inscriptions on bones and tortoise shells. The Yellow Emperor's Internal Classic (Qin dynasty and Han dynasty) and Treatise on Diseases (by Zhang Zhongjing, East Han dynasty) establish the theoretical basis of TCM, and guided the clinical practice of the medicine. Medicine and drugs are inseparable. Chinese herbal medicine has a long history as the one of TCM. Over a hundred of herbal medicines and treatment and/or prevention for dozens of diseases are registered in Canon of mountains and Sea (3rd century BC). Historical Record carries the following message " Shen Nong (the god of agriculture) tasted hundreds of herbs and initiated the medicine". Shen Nong is certainly a legend character. However, Shen Nong's Herbal Classic is a reality. It carries 365 kinds medicines from herbal, animal and mineral origins. The newly-revised Materia Medica (659 AD) was implemented in Tang dynasty. In 1578 , the well-known Compendium of Materia Medica was completed by Li Shizhen of Ming dynasty, and printed the cut blocks in 1593. After founding of new China, the Academy of Traditional Chinese Medicine, affiliated to the Ministry of Health, was set up in 1955. In 1983, seven WHO collaborating centers for TCM in China were established. The Institute of Chinese Materia Medica, China Academy of TCM is one of them.
In 1960's, malaria was epidemic when Vietnam was in the flames of war. It has been an urgent need for new antimalarial drugs due to the problem of chloroquine-resistant strains of P. Facliparum. Globally, hundreds of millions of people were annually suffered from the disease, and the mortality was increased sharply. A large scale screening for antimalarial drugs was carried out home and abroad at that time, without satisfactory results. Our project for developing new antimalarial drugs was set up under the above mentioned situation in 1969. Malaria is a common disease for the world, and recorded in a medical literature (12 century, BC) in China. I graduated from the Department of Pharmacy, Beijing Medical College, and systematically studied TCM after employed. I firmly believe that TCM with this long history is a great treasure-house, and efforts should be made to explore its essence. On the basis of collection and analysis of traditional prescriptions, over two hundreds of herbs and three hundreds and eighty abstracts from them were screened by malarial models of mouse or monkey. The screening showed positive results in October, 1971. We isolated and purified the effective compound from the traditional Chinese herb, Artemisia annua L, in 1972. It was named Qinghaosu after the herb's pronunciation in Chinese. Qinghaosu showed 100% inhibition to malaria parasites for monkey and mouse. In 1973, clinical trials verified the efficacy of Qinghaosu. A new antimalarial drug was finally appeared. Qinghaosu is a compound of sesquiterpene lactone with a peroxide. It is just what we were looking for - the antimalarial drug with totally new chemical structure. The antimalarial effect of Artemisia annua L was firstly described in "The handbook of prescriptions for emergencies" compiled by Ge Hong (281-340 AD), the physician and alchemist in East Jin dynasty. The invention of Qinghaosu is benefited from TCM. It is a good illustration of the treasure and essence in TCM and the potential for contribution to the world medicine. Qinghaosu is a drug with high efficacy, fast-action and safe. In October of 1981, I delivered a talk on the chemical research of Qinghaosu during the international symposium of Qinghaosu held in Beijing. The talk evoked great attention. Qinghaosu was appreciated as "a new antimalarial drug with importance of pointing direction for drug synthesis and design". New drug certificate for Qinghaosu was issued as the first category drug in 1986, and the one for dihydro-Qinghaosu later on. Dihydro-Qinghaosu is a derivative of Qinghaosu with two hydroxides. It provides basis for further development of derivatives of Qinghaosu. The achievements gained the National Invention Award and the Top Ten National Award for Progress in Science and Technology accordingly.
For our good wishes, the 21st century should be a better one with magnificent prospects. Although we can roam in the heavens, and the world is connected closely by the internet, but we still have to face the cruel facts of local wars and life-threatening diseases. Malaria is still a dangerous enemy to mankind in the new century. An airplane crash may kill hundreds of people, and results in an impact of shake and grief for the living people for a long time to come. However, we sometimes neglect the significant tragedy. Malaria, as the tropical disease, is cruelly killing the poor people in the developing countries. Some 500 million infections are globally reported, and some 3,000 children are killed daily in Africa only. The simple figures tell us that ten abuses [editors note: Airbuses probably] full of children were crashed every day. What a nightmare to the mankind! We get to fight back. "Roll back malaria" is the fighting target for the new century setup by WHO. I believe Qinghaosu and its derivatives are the right weapons for the combat. We sincerely hope that the invention of Qinghaosu will save thousands of endangered people from the verge of death daily. Research Center for Qinghao and Qinghaosu was established at the China Academy of TCM due to the invention of Qinghaosu. The center carries out systematic researches on Qinghaosu, and gains new progresses in compound prescriptions with better therapeutic efficacy ( increased 7.6 folds ) and in new applications of Qinghaosu. We are looking forward to cooperating with our African colleagues. I heartily hope that Qinghaosu will contribute more for the benefit of human health in the 21st century and for the bright future of mankind.
"
Thursday, June 4, 2020
Thursday, April 30, 2020
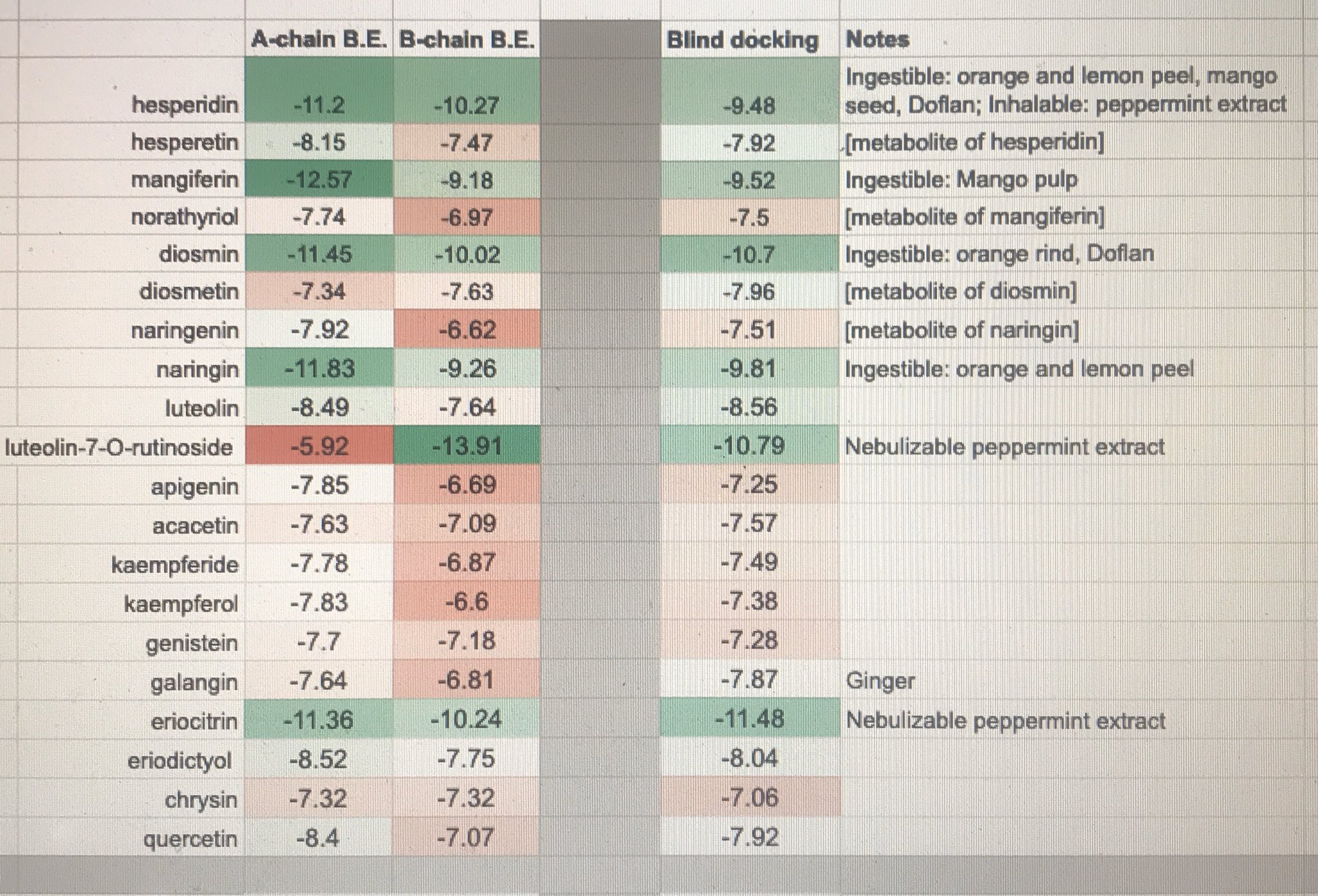
45 Flavonoids vs. SARS-CoV's 3CLpro under Autodock Vina
In Silico effect of Flavonoids on SARS-CoV 3CLpro progressively targeting A and B-chains' HIS41-CYS145 interfaces
Results:

Micro-discussion:
So while I've been a very strong proponent of Hesperidin based on in vitro results. benign cytox values, inherent known safety, and wide suppy availability, this Autodock Vina docking study shows stronger hits in 1. Hinokiflavone, 2. Luteolin-O-7-rutinoside, 3. Eriocitrin, 4. Sulcatone A, and 5. Amentoflavone.
As amentoflavone is the only one of the above with known outperforming in-vitro efficacy demonstration on SARS-CoV 3CLpro, while showing two orders of magnitude margin for cytotoxicity on Vero cells, I advocate that in vitro trials targeting phytotherapies focus on amentoflavone as applied to (e.g. e.coli-expressed) SARS-CoV-2 3CLpro proteins.
Source data:
https://docs.google.com/spreadsheets/u/1/d/19RGHp9ls3fdjDPYgT-YtNwWXsMwI9f3Glqz6KnedK0M/edit?usp=drive_web&ouid=117587353864850994495
PDB File: 2duc.pdb
Ligand Files: PubChem 3D Conformers
Citations:
Yu Wai Chen, Chin-Pang Bennu Yiu, Kwok-Yin Wong, (Hong Kong Polytechnic University)
“Prediction of the SARS-CoV-2 (2019-nCoV) 3C-like protease (3CLpro) structure: virtual screening reveals velpatasvir, ledipasvir, and other drug repurposing candidate”, F1000Research, 2020
O. Trott, A. J. Olson,
“Prediction of the SARS-CoV-2 (2019-nCoV) 3C-like protease (3CLpro) structure: virtual screening reveals velpatasvir, ledipasvir, and other drug repurposing candidate”, F1000Research, 2020
O. Trott, A. J. Olson,
AutoDock Vina: improving the speed and accuracy of docking with a new scoring function, efficient optimization and multithreading, Journal of Computational Chemistry 31 (2010) 455-461 DOI 10.1002/jcc.21334
“Anti-SARS coronavirus 3C-like protease effects of Isatis indigotica root and plant-derived phenolic compounds", Antiviral Research, Volume 68, Issue 1, October 2005, Pages 36-42.
Ryu, YB et al. (Korea Research Institute of Bioscience and Biotechnology)
"Biflavonoids from Torreya nucifera displaying SARS-CoV 3CL(pro) inhibition.", Bioorg Med Chem., 2010 Nov 15; 18(22):7940-7.
DOI 10.1016/j.bmc.2010.09.035
Michel F. Sanner.
Python: A Programming Language for Software Integration and Development. J. Mol. Graphics Mod., 1999, Vol 17, February. pp57-61
Morris, G. M., Huey, R., Lindstrom, W., Sanner, M. F., Belew, R. K., Goodsell, D. S. and Olson, A. J. (2009) Autodock4 and AutoDockTools4: automated docking with selective receptor flexiblity. J. Computational Chemistry 2009, 16: 2785-91
Wednesday, April 29, 2020
SARS-CoV-2 3CLpro- Flavonoids - (Autodock 4)
So I've been doing a lot of flavonoid in silico docking runs on SARS-CoV-2's 3CLpro (pdb file 2duc) protein. Posting results here for posterity.
Monday, April 13, 2020
One instance of research papers permalink list
(for storing, not for reading)
https://drive.google.com/file/d/1Rs9gNn_VTOZBtO5Ffmg5veTUR34PaO9u/view?usp=sharing
https://drive.google.com/file/d/1fVADH8AmlOLTkP7GkTcMTXMH8QYFRsvq/view?usp=sharing
https://drive.google.com/file/d/1uY2PICUp0RdNvwM4k_FwNuVw2hXyOCIQ/view?usp=sharing
https://drive.google.com/file/d/1mHITkOY22LYs2d89_vyRBeAqOOF6a0rQ/view?usp=sharing
https://drive.google.com/file/d/1mPD8o4JVDCLAu-P8eiObxboOyiSJrsvb/view?usp=sharing
https://drive.google.com/file/d/1tQVb8a-r-gEs8yFpO2bdJ6KalRn87ykj/view?usp=sharing
https://drive.google.com/file/d/1Rs9gNn_VTOZBtO5Ffmg5veTUR34PaO9u/view?usp=sharing
https://drive.google.com/file/d/1fVADH8AmlOLTkP7GkTcMTXMH8QYFRsvq/view?usp=sharing
https://drive.google.com/file/d/1uY2PICUp0RdNvwM4k_FwNuVw2hXyOCIQ/view?usp=sharing
https://drive.google.com/file/d/1mHITkOY22LYs2d89_vyRBeAqOOF6a0rQ/view?usp=sharing
https://drive.google.com/file/d/1mPD8o4JVDCLAu-P8eiObxboOyiSJrsvb/view?usp=sharing
https://drive.google.com/file/d/1tQVb8a-r-gEs8yFpO2bdJ6KalRn87ykj/view?usp=sharing
Subscribe to:
Posts (Atom)